Clinical particulars
24-year-old female underwent a hamstring ACL reconstruction in 2006 which was complicated by significant stiffness in the knee, and subsequent graft failure. She underwent a revision ACL reconstruction in 2009 using a patella tendon graft. Although movement returned, she never fully trusted her knee and had ongoing symptoms of instability.
In 2012, her knee gave way when she got up from a chair, resulting in swelling and a worsening feeling of instability.
In 2016, she had an MRI scan and then underwent an arthroscopy that confirmed the revision graft had failed and there was an associated meniscal tear. She experienced regular instability with pivoting movement during activities of daily living and had been unable to return to any sports activities. She was subsequently referred to another hospital where assessment confirmed an ACL deficient knee with positive Lachman and pivot shift tests. She had full movement, normal alignment, normal musculature, and examination of the other knee ligaments was entirely normal.
AP and lateral x-rays showed two non-anatomical femoral tunnels and a double tibial tunnel creating a large cavity within the proximal tibia (Fig. 1, 2).
A CT scan confirmed mal-position of the femoral tunnels, and showed the double tibial tunnel had caused a cavity with a diameter measuring at least 1.7 cm (Fig. 3). The aperture on the joint surface was in a good position and was not expanded.
Treatment
Revision surgery was planned using a hamstring graft from the opposite leg.
Arthroscopy showed there was a non-repairable medial meniscal tear that was resected and the joint surfaces were in good condition. One of the femoral tunnels was very anterior (type III tunnel), but the second femoral tunnel was close to the anatomical position (type II) and would result in breakthrough upon drilling an anatomical femoral socket.
Single stage revision ACL reconstruction was possible by filling the type II femoral tunnel and the tibial cavity with genex, after clearing graft debris and then drilling tunnels in an anatomical position. An arthroscopic photo (Fig. 4) shows the new femoral socket partly overlaps the previous tunnel that was filled with genex.
Outcome
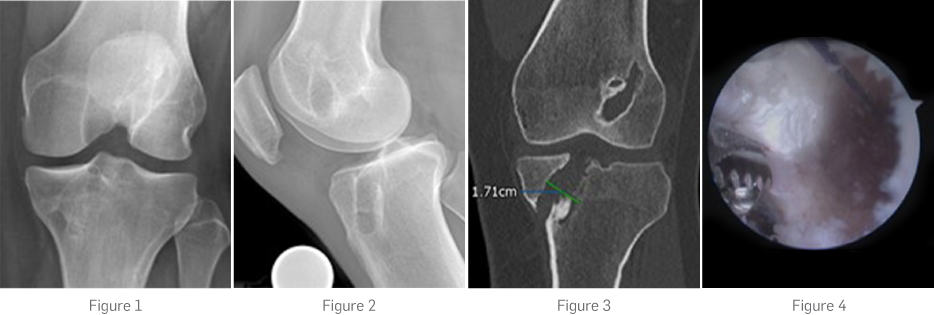
Post-operative x-rays (Fig. 5, 6) show graft fixation with a suspensory button on the femur, and a bioabsorbable interference screw and soft tissue staple on the tibia. genex filling the tunnels of the distal femur and proximal tibia can easily be seen (arrows).
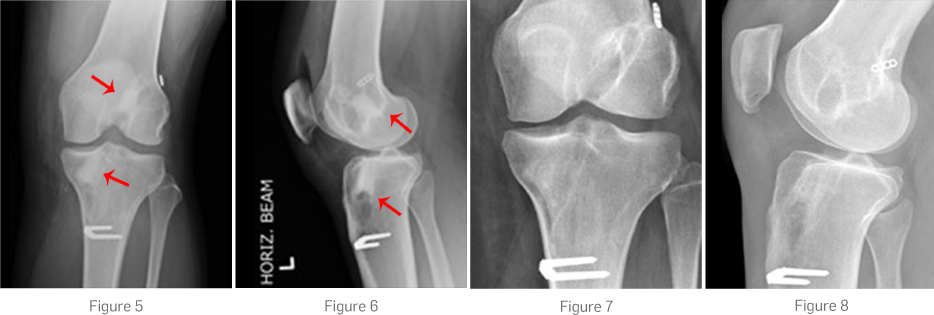
Post-operatively x-rays at seven months show bone reformation of the genex (Fig. 7, 8).
Rehabilitation was possible as for a primary ACL reconstruction, and clinical examination up to two years post-operatively showed normal ACL examination and return to normal day-to-day and some pivoting sports activities. Note: See genex page for regulatory statements. MA0358R1