Infected sacral pressure ulcer
Courtesy of Timothy Wat, Tissue Viability Clinical Nurse Specialist, West Hertfordshire, UK
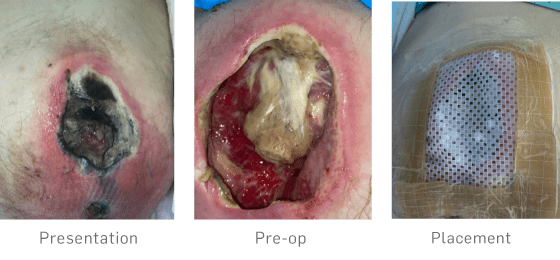
58-year-old male, paraplegic with a T4 spinal cord injury sustained 27 years ago following a road traffic collision. He was wheelchair-bound, with a background of non-diabetic hyperglycaemia and a history of smoking. He was admitted to the local acute hospital following an urgent GP referral for a suspected infected sacral pressure ulcer. He presented with a Category 4 sacral pressure ulcer, showing clear signs of wound infection. MRI confirmed osteomyelitis involving the S3–S5 vertebrae and coccyx. The wound was extensive, measuring approximately 7 cm × 4 cm with a depth of 3 cm and multiple areas of undermining. He commenced on IV flucloxacillin, which was later escalated to IV ceftriaxone for the treatment of osteomyelitis.
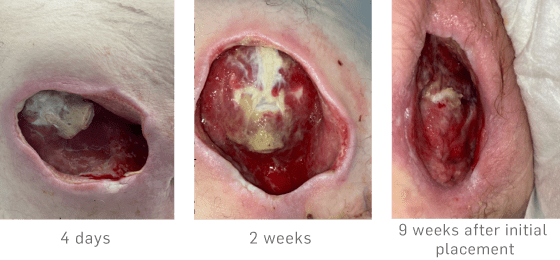
Initially, conservative sharp debridement was performed by the Tissue Viability Nurse (TVN) to reduce bioburden and remove devitalised tissue. 9 days later, 10 cc of STIMULAN, mixed with antibiotic and made into beads, was packed into the cavity to help treat the osteomyelitis. Over the next week, the STIMULAN beads were required to be topped up due to faecal contamination risk.
After 2 weeks, most beads had either dissolved or were removed. Wound management was transitioned to antimicrobial alginate. The wound had reduced in size and there was increased granulation.
After 9 weeks the wound measured 5 cm × 3 cm × 2 cm, with 100% granulation tissue. 2.5 months after the initial treatment, the patient sadly passed away. The use of STIMULAN significantly supported osteomyelitis treatment and local infection management, facilitating meaningful wound improvement and symptom relief in his final months. Notably, healing progressed from exposed bone with heavy undermining to a granulated wound bed with reduced depth and size.
Listed below are 4 of the most relevant articles for this piece but there is much more to explore on our Library page.
Explore Library